What is a UB 04 Form
A UB 04 Form is a document used to bill for all inpatient, outpatient, and emergency room services. Dialysis clinics, nursing homes, free-standing birthing centers, residential treatment centers, and hospice services are all billed using the UB 04 claim form. IHS and Tribally-owned and/or operated 638 facilities can also submit claims requesting reimbursement at the All-Inclusive Rate using the UB 04.
Information Required on the UB 04 Claim Form
Before receiving money in compensation for rendered services as a healthcare facility, you have to provide the following information appropriately:
- Healthcare service provider data
- Patient control number
- Type of bill
- Federal tax number
- Duration of the billing period
- Patient's details such as birthdate and address
- Source of referral for admission
- Service dates and units
- Total cost
- Insured's unique ID.
- Diagnosis details
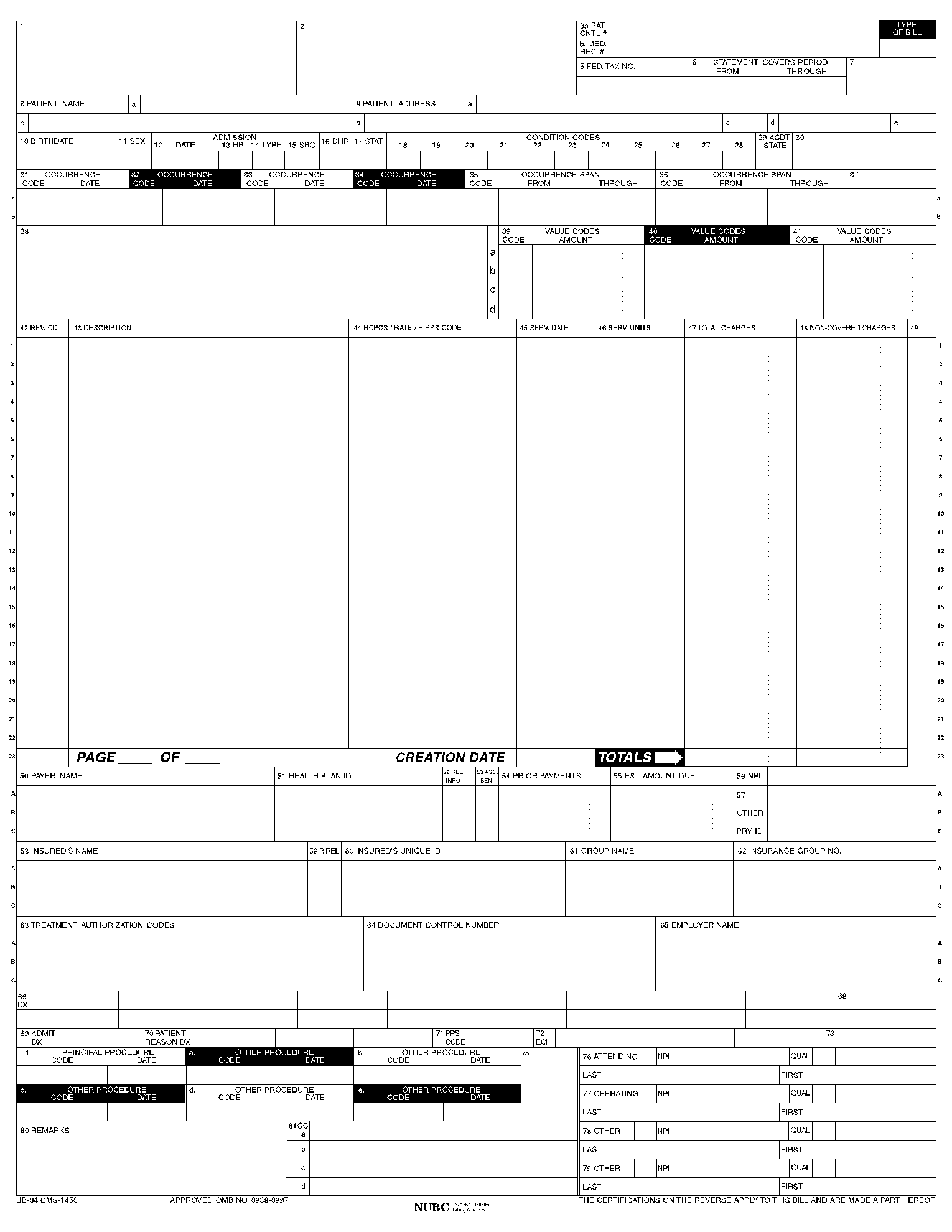
How to Fill the UB 04 Form
Satisfactory filling of the UB 04 form leads to immediate results in compensation claims. As a result, exercise the utmost care in completing the form. The following is a step-by-step to guide you on filling out the form successfully:
Step 1: Fill out the Provider Data
In the first section, enter the healthcare provider's name and address. If their pay-to address differs from the first one, provide it in the following area. In section 3, make sure you enter the unique patient number. Fill sections 4-6 with the type of bill, your facility’s federal tax number, and the billing period's duration covered by the statement, respectively.

Step 2: Fill out the Patient's Details
Enter the patient's name, identification number, and address. Give the patient's birthday, sex, date of admission, and priority of admission; for example, state whether it was an emergency or trauma, as may be the case. Next, indicate the point of the patient's origin for the admission, their discharge status, and condition codes where applicable. To conclude this step, provide the occurrence span codes, name and address of the party responsible, value codes, and amounts.

Step 3: Complete the Financial Details
If applicable, describe the services provided using the appropriate four-digit revenue code, report the revenue code, and enter your facility's appropriate CPT/HCPCS code. You have to indicate the service dates and units of all services. Provide the total charges, including non-covered costs, as shown below.

Step 4: Fill out Insurance Details
Enter the name and identification number of each payer who may have full or partial responsibilities for the charges incurred by the member. Provide your facility's ID number as assigned by the insurance companies listed and any previous charges they have met. You must provide the NPI number, the insured's unique ID, and the DX (Diagnostics and Procedure Code Qualifier). Enter the Principal ICD Diagnosis Code, the Admitting Diagnosis, the patient's reason for visiting, and the PPS code. If applicable, enter the ECI trauma diagnosis code, principal ICD procedure codes, and all providers’ full names and addresses. Under remarks, enter the CRN of the claim you are replacing and the taxonomy code.

What is the UB 04 Form Used For
You can use the UB 04 Form to bill insurance companies and Medicaid for medical and mental health claims only as an institutional health provider. Though initially developed by Medicare centers, the form has become standard to all insurance providers.
Who needs the UB 04 Form
If you are an institutional health service provider, including dialysis clinics, nursing homes, free-standing birthing centers, residential treatment centers, and hospice services, you need the UB 04 Form. IHS and Tribally-owned 638 facilities also need UB 04 Forms to submit claims. On the other hand, insurance companies require the form to process claims.
Additional UB 04 Form Resources
Below are some additional resources to help you understand this form and details to include when filling out details therein: